


1. Introduction
1.1 Background and Purpose of the Study
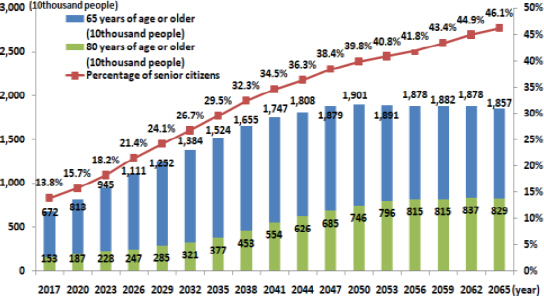
The life expectancy of the elderly population aged at least 65 years old in South Korea is steadily increasing owing to the development of advanced medical technology and the improvement of the quality of life. According to National Statistical Portal data of the National Statistical Office in 2021, the population aged at least 65 years old accounted for an all-time high of 8,125,432 (15.7%) of the entire population as of 2020, and is expected to exceed 40% of the entire population (reaching 18 million) by 2051 (Figure 1)(1). As the elderly population increases, the number of long-term care hospitals for the elderly is also increasing(2).
There are many inpatients with impaired mobility in elderly care hospitals, and it is difficult to construct fire partitions due to the nature of those hospitals due to a large number of patient rooms. Thus, the risk of spreading in the event of a fire is high, so the probability of many casualities is high.
To reduce this risk, long-term care hospitals are creating and performing fire prevention activities, such as developing their own manuals and conducting fire drills. However, such manuals and drills are written and conducted without expertise in the fields of firefighting, related facilities, construction, and evacuation in most cases. In addition, various studies(3-15) intended to assist in securing fire safety in long-term care hospitals for the elderly are limited to solving problems and improvement plans for operational and managerial elements (such as the operation and facility inspection) of these elderly long-term care hospitals. Studies regarding problems and improvement plans related to the evacuation safety of occupants (from the viewpoint of installation of firefighting facilities, and the evacuation and fire prevention elements of buildings), which are directly related to fire safety, are insufficient.
1.2 Scope and Method of the Study
In order to overcome the limitations perceived in previous studies, actual condition surveys and questionnaire surveys will be conducted with long-term care hospitals for the elderly to derive problems, and improvement plans will be presented from the viewpoint of the installation of firefighting facilities and evacuation and fire prevention elements of buildings.
To that end, for this study, two long-term care hospitals for the elderly were randomly selected in Gyeongnam, and problems related to evacuation safety, such as the management of firefighting facilities and if laws related to evacuation and fire prevention elements of buildings were applied. In addition, interviews were conducted with persons in charge of fire safety, and surveys related to evacuation were conducted with workers (caregivers, nurses, staff members, etc.). Finally, the problems that appeared in the actual condition survey and questionnaire survey were analyzed, and improvement plans were presented in this study.
2. Consideration of Problems of and Improvement Plans for Long-term Care Hospitals for the Elderly through Actual Condition Surveys
2.1 Overview of the Actual Condition Survey
Two long-term care hospitals for the elderly in Gyeongnam were randomly selected as the target sites of the actual condition survey, and an overview of the hospitals is shown in Table 1. The long-term care hospital for the elderly in K city (K hospital) has 209 beds, and it was found that the second and third floors were being used as patient rooms and were currently occupied by 190 patients. The long-term care hospital for the elderly in Y city (Y hospital) also has 199 beds, similar to K hospital, and it was found that the second and third floors were being used as patient rooms and were occupied by 199 patients.
Table┬Ā1
Overview of Long-term Care Hospital
| Type | K hospital | Y hospital |
|---|---|---|
| Building area | 1,634.77 m2 | 1,282.15 m2 |
| Total area | 6,559.14 m2 | 5,653.1 m2 |
| Floor |
Underground:1 Ground:5 |
Underground:1 Ground:4 |
| The number of beds | 209 Beds | 199 Beds |
Two firefighting engineers and two firefighting officials participated in an actual condition survey. The actual condition survey was conducted in the order of interviews with fire safety management personnel at the long-term care hospitals for the elderly, operation and condition check of firefighting facilities, checking of the operation and conditions of firefighting facilities, checking of the operation and conditions of fire doors and fire shutters, survey of the structures and actual conditions for evacuation and fire prevention, etc., in places where patients live on the floor, and factors that affect evacuation in the event of a fire.
2.2 Consideration of Problems and Improvement Plans through Actual Condition Survey
The problems derived through the actual condition survey are divided into evacuation- and fire prevention-related problems of buildings, problems related to firefighting facilities, and problems related to evacuation. The results are as follows.
2.2.1 Problems Related to Evacuation and Fire Prevention of Buildings and Improvement Plans
Problems related to evacuation and fire prevention elements of buildings identified through the actual condition survey are: 1) problems related to fire doors and fire shutters, and 2) problems related to building exit doors.
hen the problems related to fire doors and fire shutters were examined in K hospital, it was identified that the automatic opening and closing of fire doors was not difficult because of the attachment of braille blocks and hand sterilizers around the fire doors (Figure 2). Fire compartments made through the use of fire doors and fire shutters play an important role in blocking the spread of smoke and flames in the event of a fire. This is stipulated in Article 14 (Standards for the installation of fire compartments) and Article 26 (structure of fire doors) of the Rules Regarding the Standards for Evacuation/Fire Prevention Structures of Buildings. However, as shown in the results of the actual condition survey, the installation of obstacles around the fire doors is highly likely to act as obstacles to the operation and cause the failure of automatic door devices.

In order to solve these problems, improvements to devices are imperative, such as operational function inspection of items for fire doors during comprehensive precise inspection of multi-use facilities. Currently, long-term care hospitals which do not have sprinkler fire-extinguishing facilities installed but do have simple sprinklers are not subject to comprehensive precise inspections, but are subject to operational function inspection.
In addition, the door sill (Figure 3) of the integrated fire shutter, which is activated in the event of a fire, acts as an obstacle to wheelchairs and the evacuation of patients with impaired mobility. Furthermore, there appears to be difficulties in identifying these doors because of the absence of identification markers around the doors. To solve such problems, it is necessary to prepare manufacturing standards for integrated fire shutters considering the use of wheelchairs. In addition, it is necessary to prepare manufacturing standards or inspection standards (using fluorescent strips) for door identification makers.

In Y hospital, the fire doors will likely not close smoothly in the event of a fire because there is no sequential opening/ closing device for the mitergate fire doors on each floor. This is as an obstacle to the prevention of the spread of smoke and fire and the evacuation. In addition, as illustrated in Figure 4, the fire door was installed to open towards the living room rather than the exit. To solve the problems of the installation of sequential opening/closing devices for mitergate-type fire doors, the installation of these devices must become mandatory or must be added to the inspection items. In addition, the fire door needs to be installed correctly and it is necessary to prepare inspection standards to maintain and manage the opening/closing direction of fire doors.

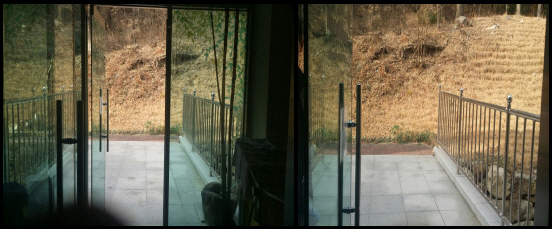
When the exit doors were examined, the width of the glass door was found to be too narrow for an intensive care bed to exit in the event of a fire.
To secure the fire safety of long-term care hospitals for the elderly, according to Article 47, Paragraph 6 of the Enforcement Decree of the Building Act, it has been stipulated since 2015 that in the case of long-term care hospitals, mental hospitals, and elderly care facilities according to Article 34 Paragraph 1 Item 1 of the Welfare of the Aged Act, residential and medical rehabilitation facilities for the disabled, separate fire-partitioned evacuation spaces should be secured, balconies for evacuation directly connected to the living room and open to the outside air should be installed, or structures in the form of viaducts should be installed to enable horizontal evacuation to the ground surface outside the building or adjacent buildings on each floor other than the evacuation floor. Currently, due to the lack of retroactive provisions related to this regulation, most long-term care hospitals for the elderly do not have fire-partitioned evacuation spaces by floor.
K hospital was not problematic in this regard because the exit door on the second floor was not designated as an evacuation space. However, the evacuation spaces by floor can be partially applied to hospitals that can secure spaces for evacuation to the outdoors without any separate fire compartments, as with K hospital.
2.2.2 Problems Related to Firefighting Facilities and Improvement Plans
Problems related to firefighting facilities identified through the actual condition survey are 1) problems in the maintenance of evacuation mechanisms, and 2) problems related to the use environment of evacuation mechanisms.
In K hospital where problems related to the maintenance and management of evacuation instruments appeared, the rescue hoses were installed on outdoor balconies, and consequently had been exposed to the natural elements for a long period of time, so their condition deteriorated (Figure 5), and were found to be in a state of high risk. To improve this state, it is necessary to secure the airtightness of the rescue hose storage box and take measures to prevent rainfall infiltration; in particular, rescue hoses should be utilized during regular training to frequently check whether rescue hoses are usable.

In Y hospital, where problems related to the environment in which the evacuation mechanisms are used, the locking device for the rescue hoses had to be unlocked using the password for the safety of patients. According to the results of the actual condition survey, it was determined that the password was shared among all staff members (Figure 6).

2.2.3 Evacuation-related Problems and Improvement Plans
The evacuation-related problems identified through the actual condition survey were 1) the absence of a horizontal evacuation plan, and 2) the insufficient number of working staff members compared to the number of patients.
When the problems related to the absence of horizontal evacuation plans were examined, it was found that the patient rooms of both hospitals were located on the second and third floors, and the numbers of critically ill patients in K and Y hospitals were 24 and 74, respectively. Despite the probability that a lot of time would be taken for many critically ill patients to evacuate through stairs, neither hospital has any horizontal evacuation plans.
The Building Act stipulates the preparation of evacuation spaces by floor in 2015, but there is no retroactive provision. However, in K hospital, it was found that despite the fact that external passages by floor were secured as with the external passage on the second floor shown in Figure 7 and the external passage on the third floor shown in Figure 8, no evacuation plan was established using the relevant passages. For hospitals that can secure spaces for evacuation to the outdoors, it is necessary to prepare a plan to partially apply the evacuation spaces by floor.

The problems related to the worker-patients ratio were found to appear more largely at night than during the day - there were more patients than workers. In K hospital, the number of working hospital staff was 66 during the day shift and 20 at night, to 24 hospitalized critically ill patients (patients who were unable to walk on their own and needed oxygen supply, EKG monitor, bed, patient transport car, etc.). Although evacuation can be carried out by moving the beds in teams of two persons or moving patients using stretchers during the day shift, at night, more resources will be needed to evacuate critically ill patients because of the insufficient number of working staff members.
In Y hospital, although the number of workers was 100 during the day shift and 74 at night, which were larger compared to K hospital, the number of critically ill patients was 72. T were patients using wheelchairs;, 107 patients were unable to walk on their own. In cases where these patients had to be evacuated vertically through stairs using stretchers, even with the current number of workers, evacuation would still be time consuming. Therefore, measures to reduce the evacuation time, such as horizontal evacuation, should be presented.
Currently, the number of workers in the two long-term care hospitals for the elderly meets the standards stipulated in Article 38 (prescribed number of medical workers, etc.) of the Enforcement Regulations of the Medical Service Act; however, because the related standards were not established considering evacuation safety, the evacuation safety cannot be wholly be secured for all patients. To solve such problems, it is necessary to verify the appropriateness of the number and arrangement of workers and establish an evacuation plan through fire safety evaluations by the hospital.
3. Derivation of Problems and Improvement Plans for Long-term Care Hospitals for the Elderly through Surveys
3.1 Overview of the Survey
The survey was conducted with caregivers, nurses, and hospital staff members working in individual hospitals and the survey comprised 17 items, including personal data, the present condition and number of patients managed by the respondent, smooth evacuation, response actions in the event of fire, initial fire extinguishing, and evacuation training.
A total of 164 respondents (80 from K hospital and 84 from Y hospital) participated in the survey.
Of the survey respondents, 19 were males (6 in K hospital, 13 in Y hospital) and 145 were females (74 in K hospital, 71 in Y hospital). In terms of age groups of the survey respondents, the number of respondents aged between 50 and 59 years old and 60 and 69 years old accounted for the largest portion of the respondents: 60 (K hospital 34, Y hospital 26) and 48 (K hospital 24, Y hospital 24), respectively. The number of respondents aged between 20 and 29 years old was shown to be 20 (K hospital 9, Y hospital 11), 60years old or older was 19 (K hospital 6, Y hospital 13), and those aged between 30 and 39 years old was 16 (6 in K hospital, 10 in Y hospital).
3.2 Consideration of Problems through Survey and Improvement Plans
For smooth evacuation, it is important to secure the minimum evacuation distance depending on the mobility of patients hospitalized in long-term care hospitals. Therefore, when asked if patients can be placed in patientŌĆÖs rooms according to mobility, 86% of respondents from K hospital and 98% of respondents from Y hospital believed it is possible. This means that if fire safety quantitative data of each hospital are provided, it is possible to arrange patientsŌĆÖ rooms to meet optimum fire safety standards.
When asked about evacuation plans by patient type (general patients, mild case patients, critically ill patients), and who should be evacuated first in the event of fire (Figure 9), 38% of the respondents from K hospital answered patients with impaired mobility (critically ill patients) ; while 36% of respondents answered mild case patients who could evacuate only when helped should be evacuated second. Among the respondents from Y hospital, 58% answered that general patients who could walk on their own should be evacuated first priority, and 33% answered that mild case patients who could evacuate only when helped should be evacuated second.

These results were compared to the fire response manuals provided by the hospitals. Although K hospitalŌĆÖs manual indicated that general patients should be evacuated first followed by mild case patients and critically ill patients in order of precedence, the largest number of respondents answered that critically ill patients should be evacuated first. On the other hand, in Y hospital, although there are evacuation plans by patient type, there is no mention of priorities by patient type. Although the order of evacuation by patient type was fixed in K hospital, the workers were not aware of it. In Y hospital, there were no priorities of evacuation by patient type, but the ignition floor was selected for the first evacuation to organize and operate a self-defense fire brigade.
When asked how to evacuate patients who could not walk on their own in the event of a fire (Figure 10), more than 95% of the respondents from Y hospital answered that they evacuated patients using stairs, but only 39% of respondents from K hospital answered that they use stairs. Respondents who chose ŌĆśotherŌĆÖ (31%), stipulated the most common responses of ŌĆśact as a team of twoŌĆÖ, ŌĆśstretcherŌĆÖ, ŌĆśevacuate using an emergency escape deviceŌĆÖ, and there were some who answered ŌĆśuse a descending life lineŌĆÖ. Among the respondents, 16% answered that they would give up evacuation and wait for rescue.

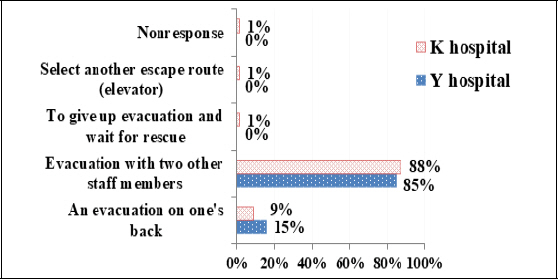
When asked about how to evacuate patients who could not walk on their own and evacuation methods using stairs (Figure 11), almost the same ratios of respondents from K hospital and Y hospital (88% versus 85%, respectively) answered that they would evacuate patients in groups of two with other staff members, and 9% of respondents from K hospitals and 15% from Y hospital answered that they would evacuate patients by carrying the patients on their shoulders or holding the patients in their arms. While most respondents from Y hospital answered that they would evacuate patients who could not walk on their own through stairs, only 39% of the respondents from K hospital answered the same. With regard to methods of evacuation through stairs, 85% of Y hospital respondents said that they would help patients evacuate in groups of two, and 15% said that they would evacuate patients by carrying the patients on their shoulders or holding the patients in their arms. Therefore, it was shown that education on the evacuation of critically ill patients who could not walk by themselves was not provided, and relevant plans were not systematically prepared in either hospital. In addition, 99% of the respondents answered that evacuation drills were necessary.
When asked what is the most worrisome in the event of a fire (Figure 12), at least 50% of respondents from both K and Y hospitals answered that safe evacuation is difficult because there were many critically ill patients.
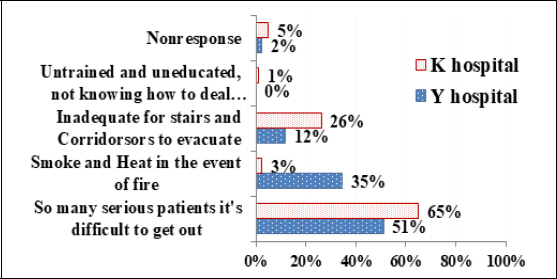
In K hospital, 26% of respondents answered that ŌĆśStructures such as stairs and passageways are inappropriate for patientsŌĆÖ evacuationŌĆÖ, and 35% of respondents from Y hospital answered that ŌĆśIt would be impossible to evacuate due to smoke and heat from the fireŌĆÖ.
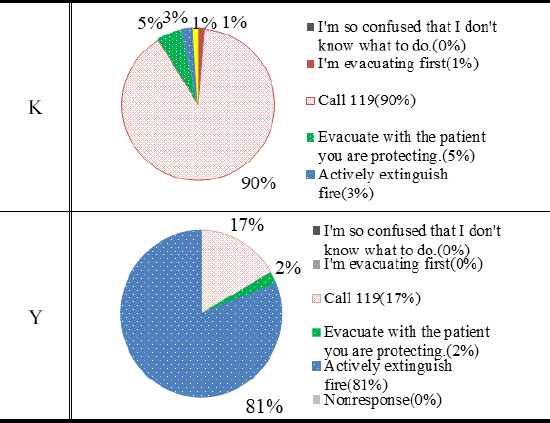
When asked about initial response in the event of fire (Figure 13), 90% of respondents from K hospital answered that they would ŌĆśreport to 119ŌĆÖ while 81% of respondents from Y hospital answered that they would ŌĆśactively extinguish the fireŌĆÖ. Therefore, it can be seen that the respondents from two hospitals are clearly divided.
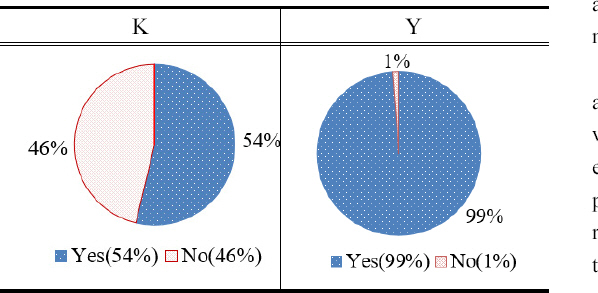
When asked about extinguishing a fire at the beginning of evacuation (Figure 14 and 15), most respondents from Y hospital answered, ŌĆśa fire extinguisher (98%), and an indoor fire hydrant (99%) can be used to extinguish the fire. In addition, all respondents from Y hospital versus 90% of K hospital respondents knew about the location and usage of fire extinguishers and indoor fire hydrants. Among the respondents, 83% and 54% answered that they could extinguish fire using fire extinguishers and indoor fire hydrants, respectively.

4. Conclusion
In this study, problems related to the evacuation of occupants and improvement plans were derived through actual condition surveys with two long-term care hospitals for the elderly.
1) The problems and improvement plans of elderly care facilities appeared through the actual condition survey are as follows:
Problems related to the maintenance of fire doors and fire shutters have been identified, and to solve these problems, it is necessary to strengthen the standards of comprehensive precise inspection for the maintenance of fire doors and add inspection items related to the opening/closing direction of fire doors, maintenance, and operation (obstacles, etc.).
In the case of problems related to outdoor doors and horizontal evacuation plans, it was found that no hospitals have retroactively secured evacuation spaces by floor or external evacuation spaces stipulated in the Enforcement Ordinance of the Building Act since 2015. In K hospital, despite spaces for evacuation to the outdoors without any fire compartment, the spaces were not applied. In this regard, it is necessary to prepare retroactive regulations related to the designation of horizontal evacuation asreas and standards related to the use of external evacuation spaces.
In the case of problems related to evacuation mechanisms, maintenance and inspection standards for evacuation mechanisms and inspection standards for securing the usability of evacuation mechanisms are deemed necessary.
Lastly, there are concerns that both hospitals will not be able to secure fire safety because of the insufficient number of workers compared to patients, and it necessary to establish evacuation plans such as appropriate numbers of workers and placement standards determined through fire safety evaluation rather than the designation of the number of workers under the Medical Service Act.
2) The problems of and improvement plans for elderly care facilities that appeared through the survey are as follows:
According to the results of the survey, the workers did not accurately recognize the evacuation order of the patients, and recognized the responses related to the evacuation of critically ill patients differently from the manual of each hospital. That is, it was found that both hospitals lacked training related to patient evacuation. It was also found that the respondents felt that it was impossible or inappropriate to evacuate patients. A fundamental review of the evacuation plans that can be carried out by current hospital workers (female or elderly workers) is necessary rather than improvement plans such as the improvement of safety education.
This study is meaningful in that it derived problems related to evacuation safety of occupants through actual condition surveys with two long-term care hospitals for the elderly and presented respective improvement plans for the problems. However, since the efficiency of each improvement plan has not been verified, it is judged that the improvement plans presented in this study should be reviewed in future studies.
Additional Remarks
This paper was prepared by modifying and supplementing Soo-Kyung ShinŌĆÖs manuscript(16) presented at the 2018 Fall Conference of the Korea Institute of Fire Science and Engineering.




